

Cleveland Clinic is one of the highest ranking and most reputable hospital systems in the United States. The nonprofit established in 1921 (Happy Anniversary!) serves over 7 million patients per year, houses the top cardiology program in the nation, and has international campuses in Canada, the UK, and the United Arab Emirates. The Cleveland Clinic rakes in around $8 billion in operating revenue per year (“Cleveland Clinic”, 2021).
Whether enough of those billions trickle down to funding quality web content is uncertain. ClevelandClinic.org is one of the top ranked health and medicine websites. One would hope to find medical information based on research, rather than propaganda and groupthink that pose a serious threat to public health.
“What You Should Know About Kratom?” a question/answer article with Dr. Yufang Lin posted to ClevelandClinic.org on June 30, 2021, presents misinterpretations, poorly researched claims, and outright falsehoods as facts. (I’m uncertain about Dr. Lin’s level of expertise on kratom, but a Pubmed search for kratom research conducted by Dr. Lin turns up no results).
The cherry on top is the condescending tone.
“People tend (however incorrectly) to think that kratom is safe because it’s ‘natural’,” the Cleveland Clinic informs us.
What people? Do they exist in large enough numbers to be addressed in a serious discussion about kratom? Most of us in the kratom community understand that we can die like Socrates if we ingest enough natural hemlock, or if we drink enough natural fermented fruit juice, or smoke enough natural opium, or get bit by a mean ol’ natural cobra snake. Many of us have even contracted a rash from natural poison ivy. Thanks for talking to us like we’re five.
The “natural” argument has been that kratom, in its unaltered state, has been consumed safely for hundreds of years. Kratom is considered safe in the cultures where it comes from, despite its manageable risks. To ignore this fact is unscientific.
“It’s also legal and easily obtainable in many states — without the stigma attached to narcotics.” Not if Cleveland Clinic can help create that stigma, right?
The article goes on to list side effects they refer to as “common” that are either extremely rare or unproven to be caused by kratom at all. I have never before heard of kratom causing “itching”, “tongue numbness” and “aggression”. If these are side effects, they’re certainly not “common”. “Altered mental status” seems like a hilariously general term, but apparently it’s used in medicine. Johns Hopkins Psychiatry Guide calls it “a vague and often misleading term that can encompass any change in a patient’s mood, behavior, psychomotor skills, and/or cognition.”
Then there’s the classic. According to the Cleveland Clinic, celebrating its 100th year of healthcare excellence, kratom causes “Delusion and hallucination.”
We tackled the widespread falsehood that kratom causes hallucinations in 2018, and tracked exactly where it came from: misinterpretations of an early study co-authored by kratom expert Dr. Chris McCurdy (Babu, 2008) about both kratom and salvia divinorum. Salvia divinorum does cause hallucinations, as noted this in the study. But the study never claimed that kratom caused hallucinations. Subsequent, poorly-researched papers referenced McCurdy’s work, claiming hallucinations as a side effect of kratom (Chang-Cien, 2017, for example). That’s what happens when you do a “Ctrl-F” to bolster your foregone conclusions instead of reading the whole paper.
Cleveland Clinic also listed “respiratory depression” under “other serious side effects” even with abundant research available that kratom alkaloids act on the mu-opioid receptors without recruitment of beta-arrestin, the mechanism responsible for respiratory depression in classical opioids. (Kreugel 2016, for example).
Claiming “psychosis” as a side effect of long-term kratom use is another doozy, as the largest study on this topic among regular, long-term kratom consumers in Malaysia “found no evidence of elevated psychosis among regular users” (Leong Bin Abdullah, 2019).
“Knock yourself out” – Cleveland Clinic extern Kyle McGrath in presenting a list of papers that don’t back up the claim that kratom has caused death
However, the most extreme statement by Cleveland Clinic in this piece is, “kratom has even caused death.” Not “kratom-related death”. Not “death associated with kratom”. But literally, “kratom has even caused death”.
Questioned on Twitter for sources, Kyle McGrath, a Cleveland Clinic research extern and the article’s apparent author/interviewer, replied “Knock yourself out” with a list of DOI links to kratom studies.
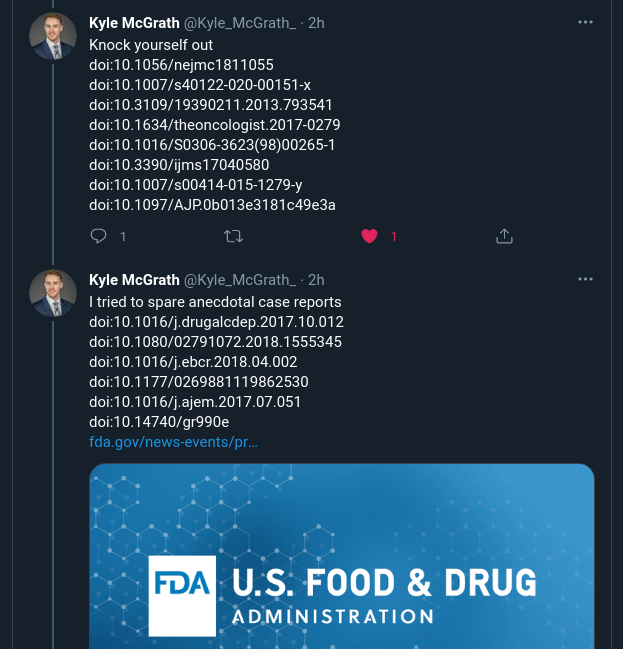
Dirk Netter, author of the first German language book devoted to kratom, decided to go through each of McGrath’s sources. Many of these were covered here on KratomScience and we’ve interviewed many of the scientists who have co-authored the papers. None of the scientists we have interviewed claim kratom is 100% risk-free, but none mentioned any evidence of any kratom-caused death. Netter went through each study and found no evidence of deaths caused by kratom alone. Please read this thread in its entirety:
Not only was there no evidence of kratom-caused death, Cleveland Clinic was using as a source the 2011 Kronstand case report of nine deaths in Sweden after ingestion of “Krypton” – a mixture of a normal dose of kratom with a deadly dose of O-desmethyltramadol. This was one of the infamous reports that FDA used to bolster its push for prohibition without citing the actual report, as documented by Jane Babin:
The FDA attributed these deaths to the use of a powdered kratom product marketed on the Internet as “Krypton”, without disclosing that Krypton is not natural kratom, but is an adulterated product contaminated with dangerous levels of O-desmethyltramadol; without citing the Case Report that first brought these deaths to their attention; without giving adequate weight to the conclusions reported in that Case Report
(Babin, 2018)
Shortly after this exchange, Kyle McGrath deleted his Twitter account.

References
(though a humble blog that constantly gets knocked out of Google ranks because we have “kratom” in the title, we occasionally cite sources, or at least link them)
Babin, JK. (2018). FDA fails to follow the science on kratom. Downloaded 5/26/21 from Wixstatic https://t.co/G76TVsWdLY?amp=1
Babu, K. M., McCurdy, C. R., & Boyer, E. W. (2008). Opioid receptors and legal highs: Salvia divinorum and Kratom. Clinical toxicology (Philadelphia, Pa.), 46(2), 146–152. https://doi.org/10.1080/15563650701241795
Chang-Chien, G. C., Odonkor, C. A., & Amorapanth, P. (2017). Is Kratom the New ‘Legal High’ on the Block?: The Case of an Emerging Opioid Receptor Agonist with Substance Abuse Potential. Pain physician, 20(1), E195–E198. https://www.painphysicianjournal.com/linkout?issn=&vol=20&page=E195
“Cleveland Clinic”. (2021, June 10). In Wikipedia. https://en.wikipedia.org/wiki/Cleveland_Clinic
Cleveland Clinic. (2021, June 30). What you should know about kratom. https://health.clevelandclinic.org/what-is-kratom/
Kronstrand, R., Roman, M., Thelander, G., & Eriksson, A. (2011). Unintentional fatal intoxications with mitragynine and O-desmethyltramadol from the herbal blend Krypton. Journal of analytical toxicology, 35(4), 242–247. https://doi.org/10.1093/anatox/35.4.242
Kruegel, A. C., Gassaway, M. M., Kapoor, A., Váradi, A., Majumdar, S., Filizola, M., Javitch, J. A., & Sames, D. (2016). Synthetic and Receptor Signaling Explorations of the Mitragyna Alkaloids: Mitragynine as an Atypical Molecular Framework for Opioid Receptor Modulators. Journal of the American Chemical Society, 138(21), 6754–6764. https://doi.org/10.1021/jacs.6b00360
Leong Bin Abdullah, M., Singh, D., Swogger, M. T., Rahim, A. A., & Vicknasingam, B. (2019). The prevalence of psychotic symptoms in kratom (Mitragyna speciosa Korth.) Users in Malaysia. Asian journal of psychiatry, 43, 197–201. https://doi.org/10.1016/j.ajp.2019.07.008
Dr. Ling
Is an Intergrative-Pediatric Physician. I can not find anything or anywhere where she has done or been involved in clinical case studies regarding Kratom. Actually with no Clinical Studies-blind trials approved by the F.D.A for study of Mitragynia in humans there is no peer review as required. She is making bias statements, but does promote the use of essential oils with Western Medicine. Since Dr. Ling is listed as an intergrative M.D. one would think she would delve into the study of this leaf without bias.
This is the biggest B S. Article Ive seen yet. Im a Cleveland Clinic patient but this article really pisses me off. As a kratom consumer and advocate, Ive never had any of these so called side effects other than itching. Guarantee the “deaths” she speaks of were from fentanyl or other drugs mixed with kratom. This article just cost them a patient.
well, tongue numbness is at least somewhat possible since some of the alkaloids in kratom act as local anaesthetics, but I don’t consider it a side effect, it’s part of the effects kratom can have when taken orally. The rest of the psychological jargon? Worthless. Thank god netter and brian dismantled this page, it was driving me nuts
Laughing so hard, thanks for talking to us like we’re five, I thought the exact same thing when I came across the cleveland clinic article. Love this! You should do more of these when new hit peaces come out